Two-stage Repair of Tetraology of Fallot
Patient Case Discussion
Loading video...
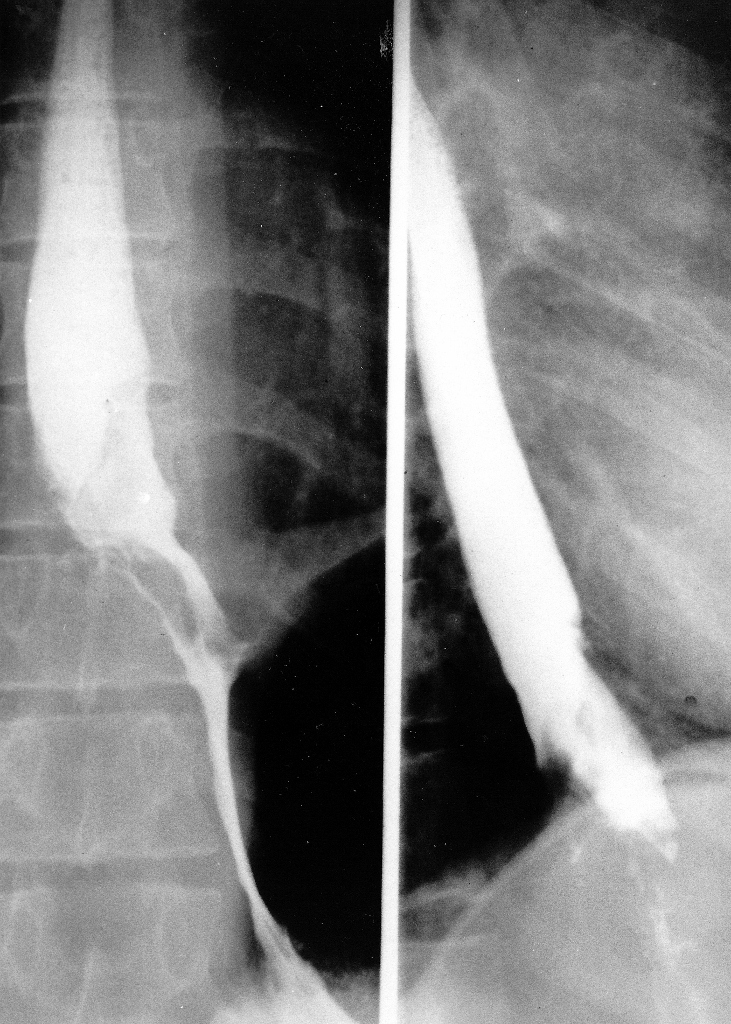
Fig. 1. Pre-Operative Barium Swallow (Select Image for High-quality Version). This demonstrates an irregular intraluminal lesion at and above the gastroesophageal junction.
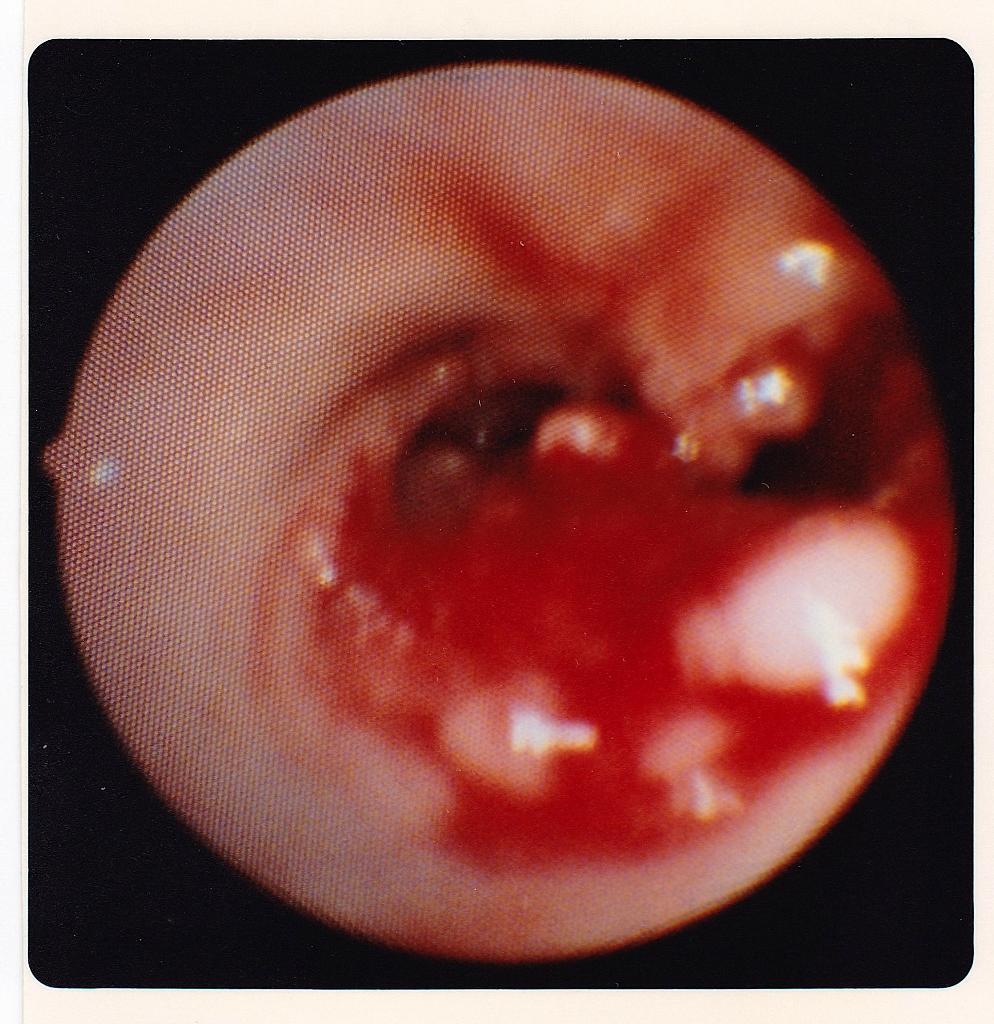
Fig. 2. Endoscopic View of Upper End of Esophagogastric Adenocarcinoma (Select Image for High-quality Version). Esophagoscopy showed an obvious carcinoma of the esophagus, a well differentiated adenocarcinoma histologically.
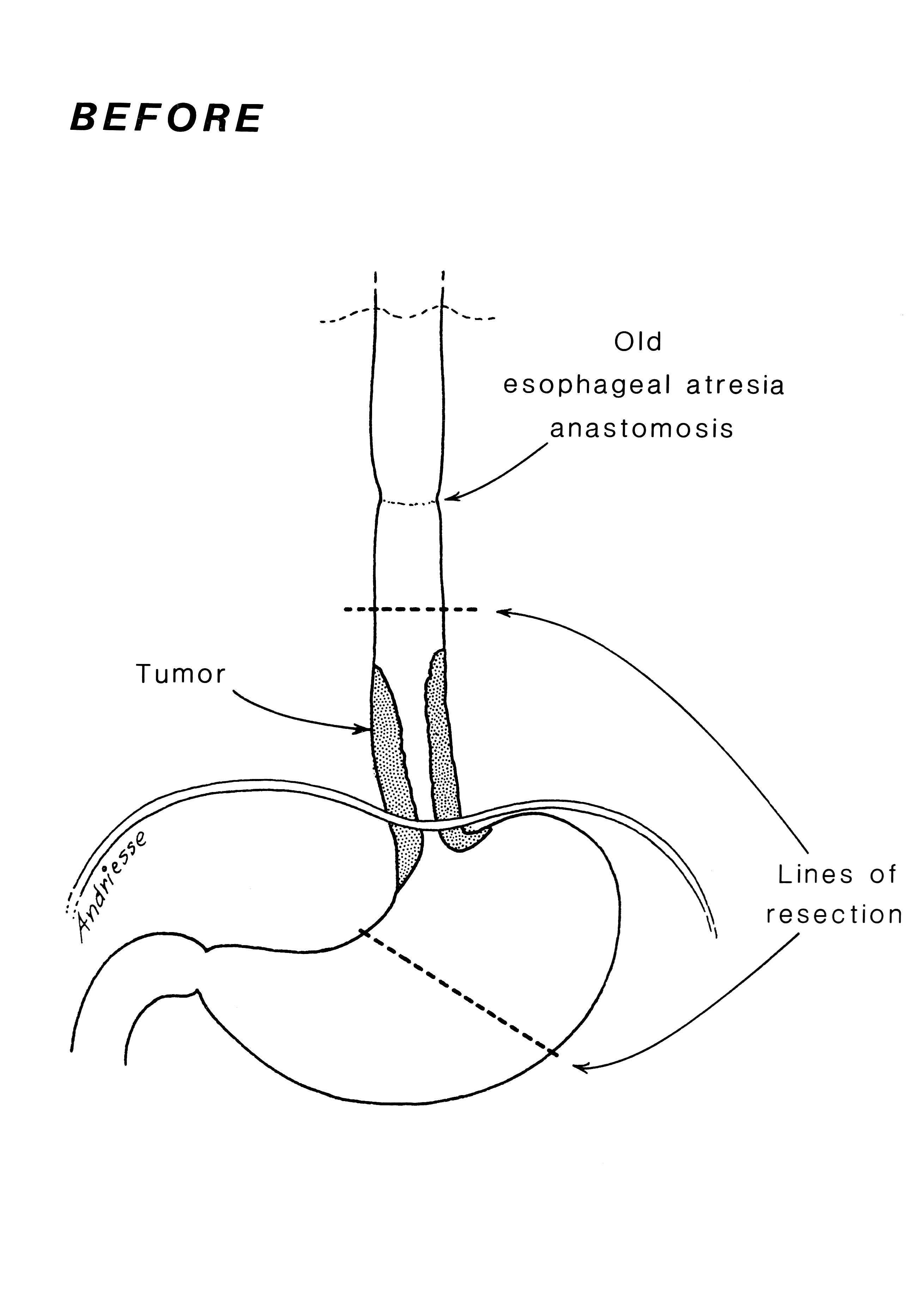
Fig. 3. Pre-Operative Anatomy (Select Image for High-quality Version). Diagram shows the extent of tumor and of resection to be performed using a thoracoabdominal exposure.
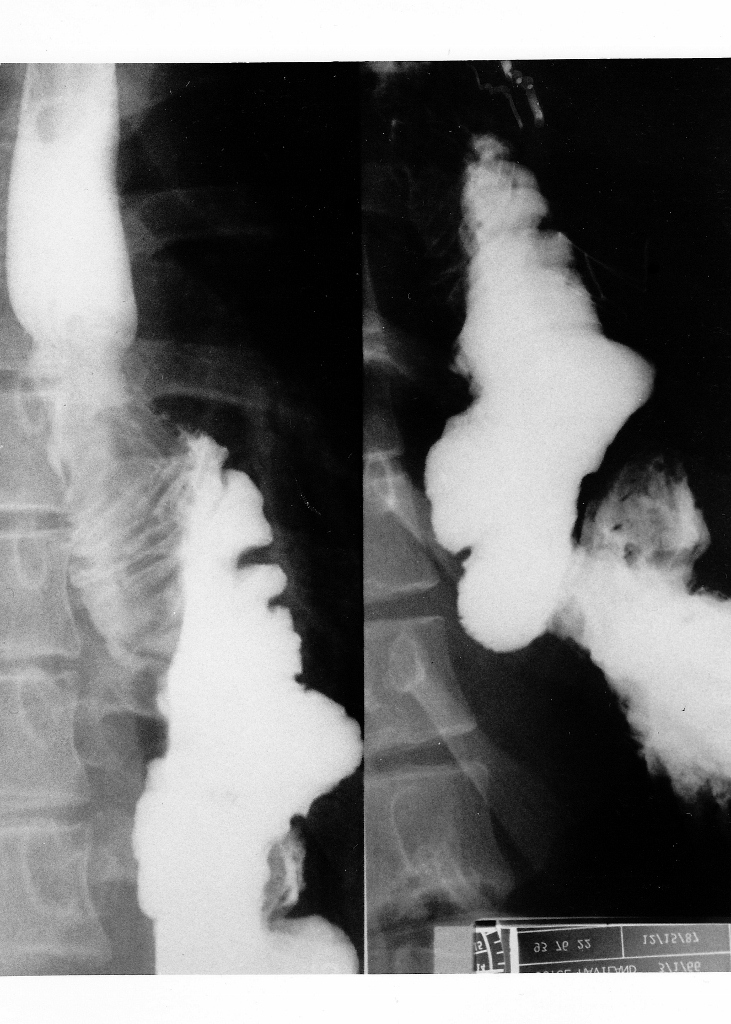
Fig. 4. Post-Operative Barium Swallow (Select Image for High-quality Version). This shows colon interposition from mid esophagus to remaining stomach.
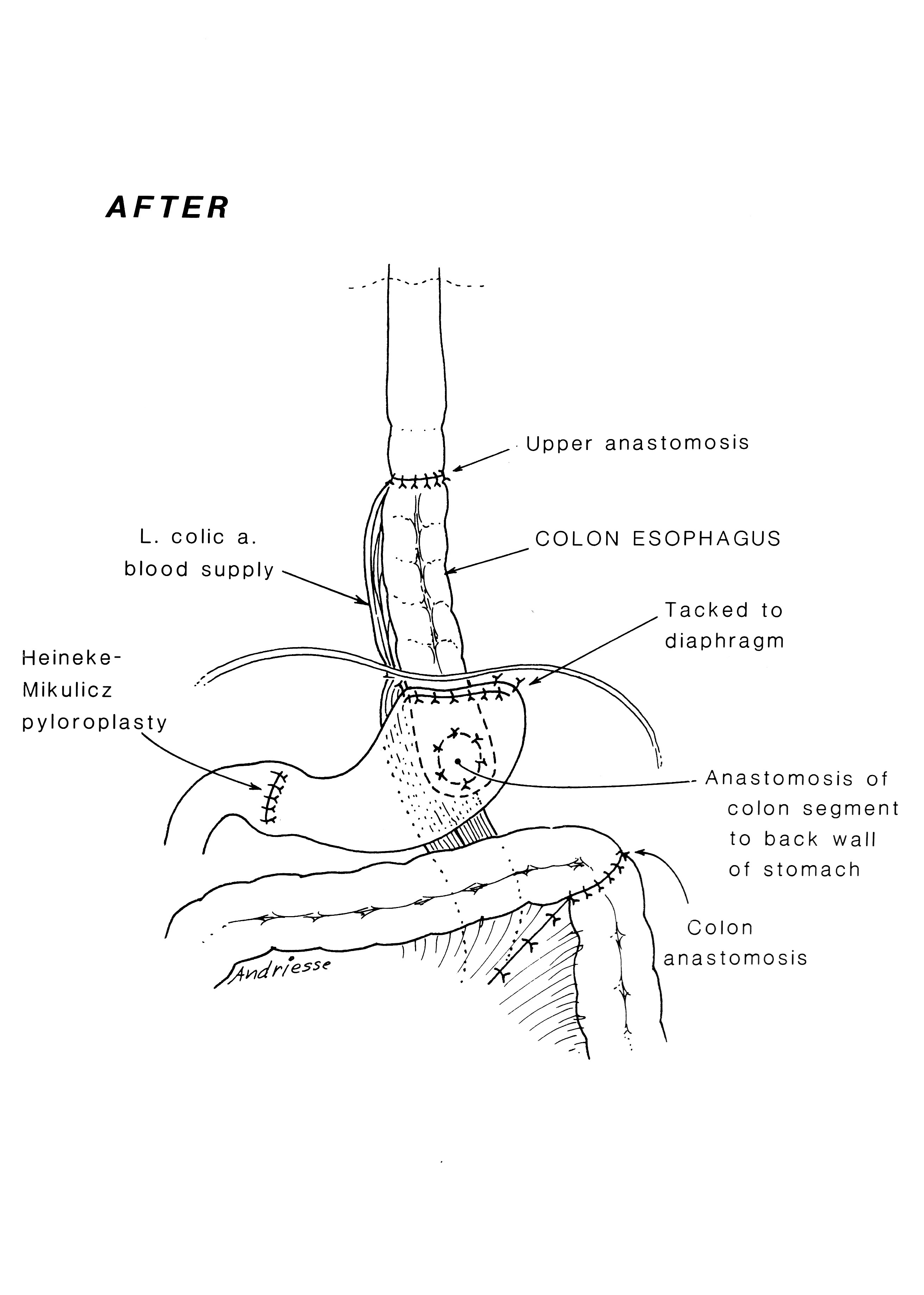
Fig. 5. Post-Operative Anatomy (Select Image for High-quality Version). Anatomy after tumor resection, and restoring gastrointestinal continuity with segment of transverse colon on left gastric pedicle. Note pyloroplasty to enhance gastric emptying.
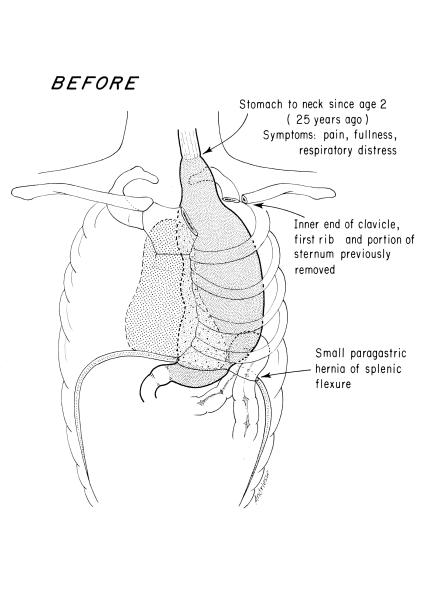
Fig. 1. Pre-Operative Anatomy. Gastric “pull-up operation” done in childhood.

Fig. 2. Barium Filled Stomach. Upper G.I. series age 28 years, with severe symptoms secondary to stomach in the thorax.
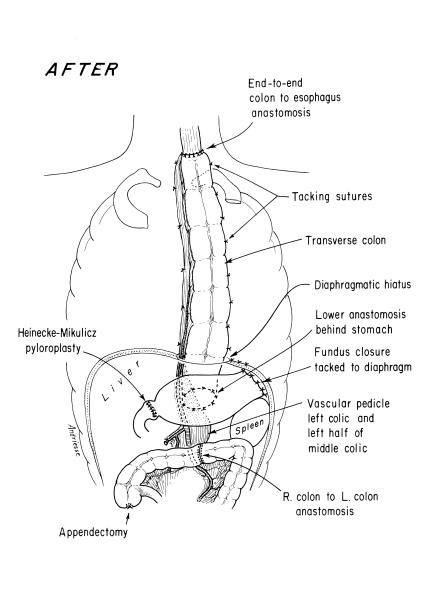
Fig. 3. Post-Operative Anatomy. Esophagoscopy immediately preceding the surgery interestingly showed no esophagitis in the segment just proximal to the gastric fundus in the upper thorax. The scope could pass easily all the way into the duodenum without encountering inflammatory changes.
One of the early survivors among 12 babies with esophageal atresia was managed by closure of the tracheoesophageal fistula (TEF), gastrostomy, and exteriorization of the cervical esophagus to the left neck as a neonate. Then a subcutaneous presternal “esophagus” was made in stages.
 n
n