This 3-year-old girl was referred for reconstructive surgery in 1988. Born with severe bilateral obstructive megaureters with hydronephrosis, bilateral end ureterostomies had been performed at age 1 month. The ureterostomies did not drain well. Therefore, bilateral loop cutaneous ureterostomies were performed at age 1 year. Hydronephrosis improved; the ureterostomies were then closed, but severe hydronephrosis recurred.
Preoperative assessment showed a very small bladder volume of only 10 ml. When contrast was introduced through the end ureterostomy stomas, the ureters drained well, but contrast remained in the kidneys, indicating functional ureteropelvic junction obstruction bilaterally.
At reoperation the better ureter on the left was reimplanted with a long tunnel into her tiny bladder, together with a psoas hitch. The right side was drained by a transureteral ureterostomy to the left. Both upper ureters were obstructed from angulation at the site of the ureterostomy closures. Therefore, bilateral dismembering pyeloplasties were performed, maintaining adequate ureteral blood supply in the surrounding periureteral tissues. The bladder was augmented with a large segment of stomach based on the right gastric epiploic artery. This 13-hour operation was well tolerated. Bladder emptying was performed initially by intermittent catheterization by her mother. Gradually she learned to void completely, and catheterization was stopped.
Postoperative studies showed some reflux. Subureteric injection of Teflon paste beneath the single ureteral orifice stopped the reflux.
Comment from Dr. Hendren: Use of the stomach for bladder augmentation has some advantages over small bowel and colon. It is metabolically superior regarding chloride absorption and base loss, seen with segments of small bowel and colon. Those segments tend to lose bicarbonate and potassium and to a lesser extent sodium while resorbing chloride. If potassium loss is replaced as potassium chloride, bicarbonate loss can be accelerated, aggravating acidosis. Gastric mucosa secretes chloride and is therefore preferred in patients with poor renal function who cannot tolerate increased solute resorption with acidosis. The urine is usually sterile after gastrocystoplasty. The ureters are tunneled very easily into gastric mucosa which is durable and also compliant. The stomach may be the only reasonable means for reconstruction in certain patients with cloacal exstrophy who have little or no colon, and who have a short small bowel in particular. Its metabolic superiority probably makes it the augmentation of choice in patients with very poor renal function. These patients also do not have excess mucous in the urine, which is an added advantage because mucous provides a nidus for stones. Cutaneous ureterostomy was a common type of diversion in infants a few years ago. It can cause many complications however, as shown in this case.


Anatomy (Select Image for High-quality Version). (Top) Pre- and (Bottom) Postop anatomy.
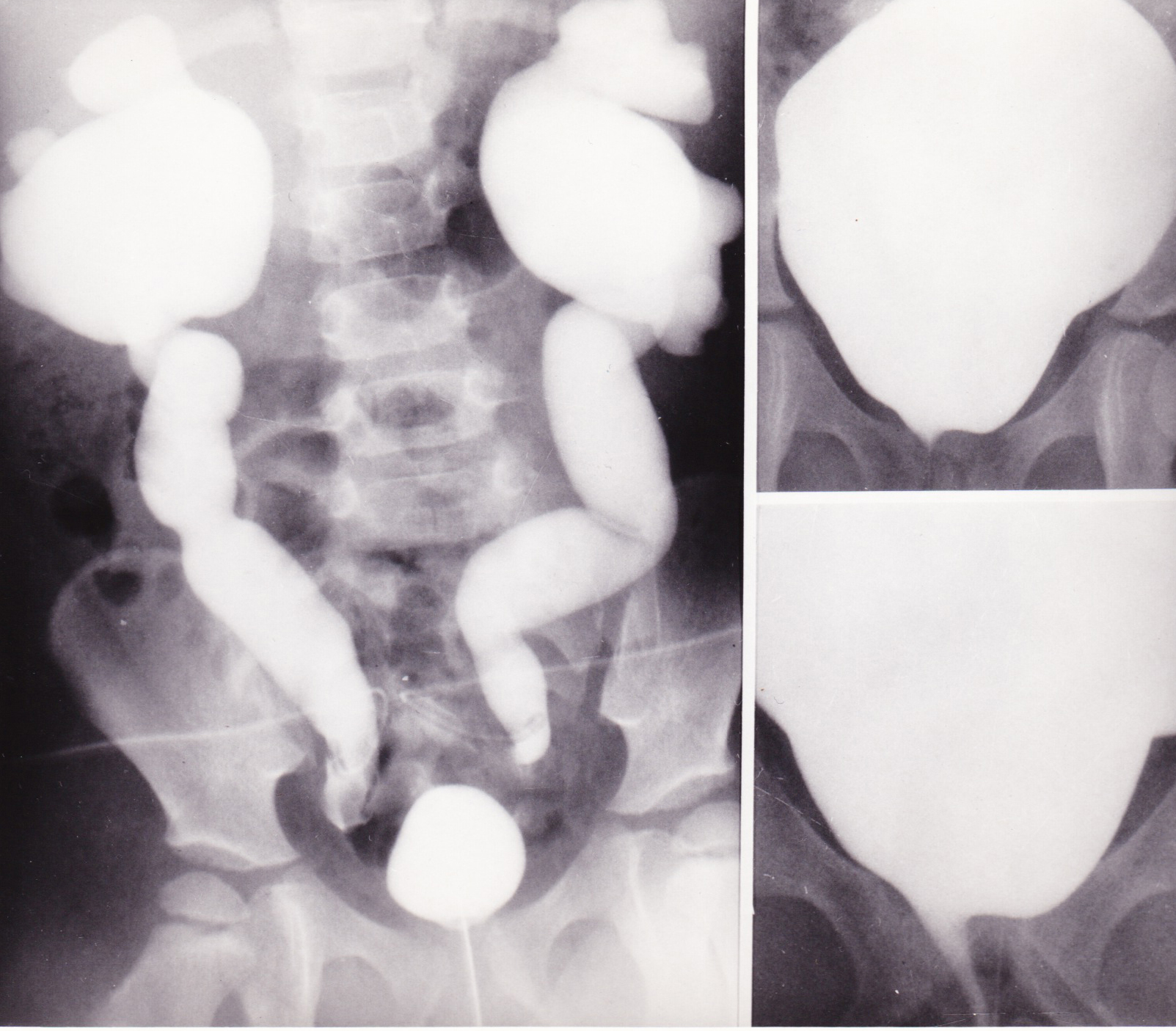
X-rays (Select Image for High-quality Version). Preoperative x-ray studies. Both kidneys and ureters filled via end ureterostomies Small bladder filled via urethral catheter.(Left) Postoperative bladder studies after gastrocystoplasty. (Top Right) After filling. (Bottom Right) Voiding cystogram with good control.

X-rays (Select Image for High-quality Version). IVP 2 years postoperatively. Note: right ureter enters left just above bladder. Both ureters greatly improved in size and emptying.
Follow up 2 years postoperatively, the patient was voiding normally, was dry and free from urinary infection. Blood chemical values were remarkably normal, considering her degree of hydronphrosis originally present: BUN 10 ml., Serum creatinine 0.3 and creatinine clearance of over 120. Urodynamic studies showed the bladder capacity then at age 5, to be 275 ml. with no uninhibited contractions and normal sphincter function. The patient is now age 28 years. She has normal urinary continence.